Anatomy of SP 4 (Gongsun) and Balance of the Medial Arch
This blog post on the anatomy of SP 4 contains an image and a video from cadaver labs in the Sports Medicine Acupuncture Certification program. These are for medical professionals only and its use is strictly for educational purposes. Do not share these with anyone who is not a medical professional or with any intention other than enhancing medical knowledge.
The anatomy associated with SP 4 (gongsun) has some very fascinating aspects, which can give insight to this point. As many acupuncturists know, SP 4 is the luo-connecting point of the Spleen channel and is the confluent point of the chong mai. The point is described as being in the depression distal and inferior to the base of the first metatarsal. In Sports Medicine Acupuncture Certification (SMAC), we palpate here and also at the joint line (metatarsal-cuneiform joint) and pick the most reactive of the two when treating.
There are many indications that acupuncturists use this point for. In addition to these common indications, acupuncturists who have studied Sports Medicine Acupuncture (SMA) also use this point, combined with P 6, as part of a comprehensive treatment for upper cervical and thoracic vertebral fixations. This blog post will look not at the actions and indications of this point as a distal point, but, instead, will zoom in and look at the structural and functional anatomy of this point. Acupuncturists will gain a different view of this point from this approach which can broaden treatment options and increase understanding of how this local region relates to the channel system.
 We can start with the anatomy associated with the point itself and notice something immediately that helps link it with the channel of its external channel pair, the Stomach channel. The tibialis anterior muscle, a muscle of the Stomach channel sinews (jingjin), travels from the Yang side of the leg just lateral to the tibial crest (following the Stomach channel), crosses at the ankle towards the Yin side (recall that this muscle is the lateral border of LIV 4), and attaches to the Yin side of the foot at SP 4. Specifically, it attaches to the medial cuneiform and base of the first metatarsal. This muscle is a physical representation of the uniting of the Spleen and Stomach channel network.
We can start with the anatomy associated with the point itself and notice something immediately that helps link it with the channel of its external channel pair, the Stomach channel. The tibialis anterior muscle, a muscle of the Stomach channel sinews (jingjin), travels from the Yang side of the leg just lateral to the tibial crest (following the Stomach channel), crosses at the ankle towards the Yin side (recall that this muscle is the lateral border of LIV 4), and attaches to the Yin side of the foot at SP 4. Specifically, it attaches to the medial cuneiform and base of the first metatarsal. This muscle is a physical representation of the uniting of the Spleen and Stomach channel network.
The tibialis anterior dorsiflexes the ankle and inverts the foot at the subtalar joint. It is this motion of the foot inversion (lifting of the medial arch) that I want to focus on for this post. It is worth mentioning that ST 36 is the motor point of the tibialis anterior and that needling this point can affect tension in the muscle.
 The tibialis posterior is another important muscle which attaches to the region. It has many attachments on the foot, including to the medial cuneiform. This muscle merges at the distal attachment with the joint capsule and with the tibialis anterior muscle to form a fascial continuity. This muscle also has a very prominent attachment to the navicular bone. Like the tibialis anterior, the tibialis posterior performs inversion of the foot at the subtalar joint.
The tibialis posterior is another important muscle which attaches to the region. It has many attachments on the foot, including to the medial cuneiform. This muscle merges at the distal attachment with the joint capsule and with the tibialis anterior muscle to form a fascial continuity. This muscle also has a very prominent attachment to the navicular bone. Like the tibialis anterior, the tibialis posterior performs inversion of the foot at the subtalar joint.
This muscle is part of the Spleen channel sinews. You can access this muscle at the motor point location, which is deep to SP 8 (this technique should be learned in a classroom setting to avoid hitting the tibial artery). Another reactive region of this muscle is at SP 6.
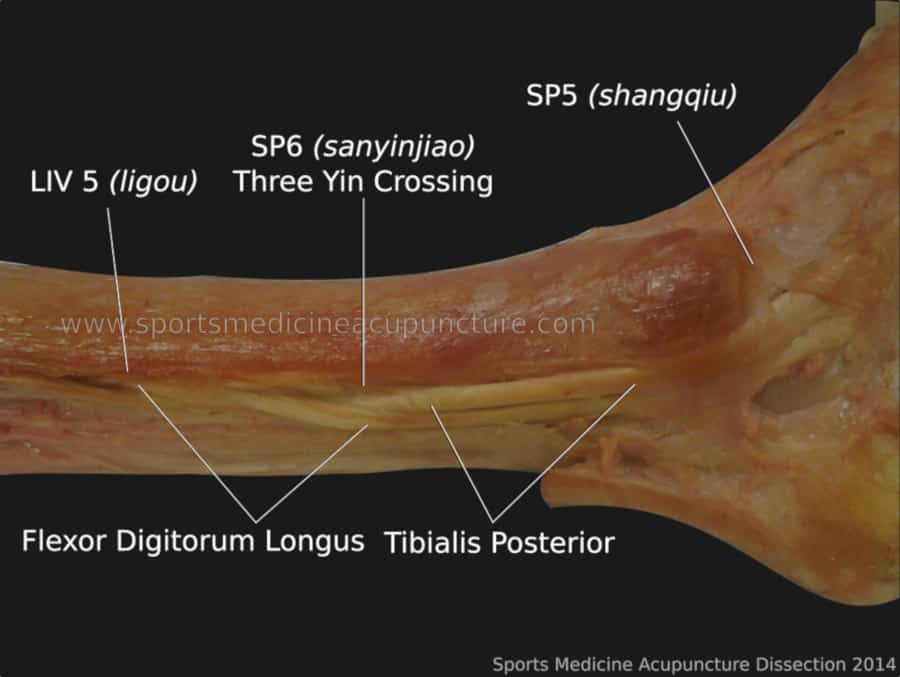
Below is a cadaver image that shows the relationship of the tibialis posterior, which proximally is the middle muscle of the deep posterior compartment, but then crosses anterior to the flexor digitorum longus (a muscle in the Liver channel sinew) at the region of SP 6. This image has the soleus (a muscle of the Kidney channel sinew) removed, but you can get a sense of how there is a physical representation of the three yin channels crossing at SP 6 (sanyinjiao). Also note the relationship of the tibialis posterior tendon to SP 5.
A collapse of the medial arch, a condition call pes planus, then can frequently involve the ‘sinews’ of the Stomach and Spleen. The Kidney channel sinews are also frequently involved, but this discussion will have to wait until another time.
Staying with the Spleen and Stomach, it is worth remembering that these two channel networks (including the primary channels and zangfu) are much more integrated than other internal-external pairs, so much so that it is sometimes difficult to separate their functions. This is even evident in the classics when the organs are assigned bureaucratic roles, a likely memory aid for early physicians to simplify and remember their functions. While the organs all have a role and brief overview, the Spleen and Stomach are mentioned together, signifying how integrated their roles are (The Spleen-Stomach holds the office of the granaries and issues the five flavors). Also, the Stomach channel is the only Yang channel on the anterior portion of the body, signifying its close relationship with the Spleen channel. The same applies to the channel sinews of these networks as the muscles involved often work together, in this case to lift the medial arch. It is actually not uncommon, and not surprising, to find signs of deficiency of these organs with patients who have pes planus. The Spleen qi in particular, which lifts, will often be weak, failing to lift the medial arch.
The final consideration for the medial arch, and SP 4 specifically, is to see what muscle is acting as an antagonist to the tibialis anterior (ST) and posterior (SP). In this case, it is the peroneus longus and brevis. The muscles would seem to be on the Gallbladder channel sinew at first glance, but if you look at any description, including the information from the Lingshu, you would see that the Urinary Bladder channel 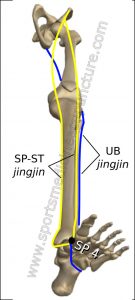 sinew has a lateral branch which travels behind the lateral malleolus. In SMAC we interpret this to be the peroneus longus and brevis. Watch the video below to see how the peroneus longus and the lateral hamstrings (a muscle obviously of the UB channel sinew) communicate tension. For this post, we are concerned with the distal end of this muscle which goes from the lateral foot proximal to UB 63, deep in the plantar foot to attach to the same place as tibialis anterior, the medial cuneiform and the base of the 1st metatarsal. This muscle, which forms a fascial sling with tibialis anterior and posterior, pulls the foot into eversion. It is assisted by the peroneus brevis. The image to the left shows a schematic. The blue represents the UB jingjin; for this discussion that would be the peroneus longus, but it also shows the fascially connected biceps femoris attaching to the back of the pelvis. The yellow shows the SP jingjin. For this discussion, that involves the tibialis posterior (SP) and tibialis anterior (ST), but also shows the channel connecting to the front of the pelvis via the sartorius (SP) and rectus femoris (ST). In SMAC we relate the foot position to the pelvic position which assists when treating many injuries.
sinew has a lateral branch which travels behind the lateral malleolus. In SMAC we interpret this to be the peroneus longus and brevis. Watch the video below to see how the peroneus longus and the lateral hamstrings (a muscle obviously of the UB channel sinew) communicate tension. For this post, we are concerned with the distal end of this muscle which goes from the lateral foot proximal to UB 63, deep in the plantar foot to attach to the same place as tibialis anterior, the medial cuneiform and the base of the 1st metatarsal. This muscle, which forms a fascial sling with tibialis anterior and posterior, pulls the foot into eversion. It is assisted by the peroneus brevis. The image to the left shows a schematic. The blue represents the UB jingjin; for this discussion that would be the peroneus longus, but it also shows the fascially connected biceps femoris attaching to the back of the pelvis. The yellow shows the SP jingjin. For this discussion, that involves the tibialis posterior (SP) and tibialis anterior (ST), but also shows the channel connecting to the front of the pelvis via the sartorius (SP) and rectus femoris (ST). In SMAC we relate the foot position to the pelvic position which assists when treating many injuries.
These three muscles of the fascial sling are able to communicate tension and are able to help balance the foot in standing and during gait where they prevent too much foot pronation as the weight falls into the foot. If there are imbalances where the peroneals are locked-short and pulling excessively up, thus everting the foot, and the tibialis posterior and anterior and locked-long and failing to lift and support the medial arch, the medial arch will collapse in weight bearing. We have specific techniques taught in SMAC that can correct this, and specific corrective exercises are then prescribed to reinforce treatment. This treatment would be applicable in painful conditions affecting the foot, ankle, knee, hip, and even higher, as the position of the foot is so involved with the biomechanics of other joints.
Check out the video on our Youtube channel to see a sample treatment performed by Matt Callison in SMAC class.
When pes planus is present, the techniques demonstrated in this video could be included as part of a comprehensive treatment for injuries, such as tibial stress syndrome (shin splints) and patellofemoral syndrome.
If you want to read more on the anatomy of SP 4, check out these notes from a lecture Matt Callison and I gave at the Pacific Symposium in 2017.
Also, you can read a related post on my blog, Anatomy of the Sinew Channels—Assessment and Treatment of the Channel Sinews: Pes Planus
To learn more about AcuSport Education’s educational offerings, go here:
About the author(s):

Brian Lau, AP, C.SMA is has been on the faculty of the Sports Medicine Acupuncture Certification since 2014, and also teaches foundation courses with AcuSport Education. Brian lives and practices in Tampa, FL where he owns and operates Ideal Balance: Center for Sports Medicine Acupuncture (www.ideal-balance.net). He blogs on anatomy and TCM at www.sinewchannels.com.
About the author(s):
Brian Lau, AP, C.SMA is has been on the faculty of the Sports Medicine Acupuncture Certification since 2014, and also teaches foundation courses with AcuSport Education. Brian lives and practices in Tampa, FL where he owns and operates Ideal Balance: Center for Sports Medicine Acupuncture (www.ideal-balance.net). He blogs on anatomy and TCM at www.sinewchannels.com.