Anterior Knee Pain: Articularis Genus and Extra Point Jianxi
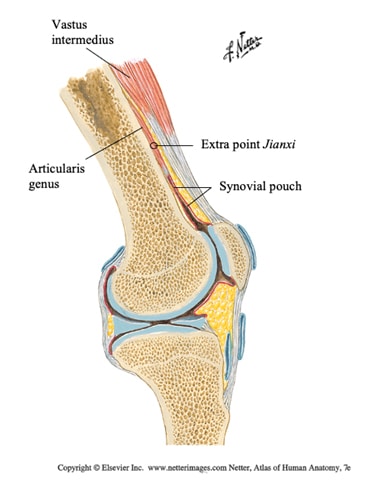 The articularis genus muscle is a thin, ribbon-like muscle of the anterior knee. It is located on the anterior surface of the distal quarter of the femur. It is deep to, and many times embedded within the fibers of the vast us intermedius muscle.
The articularis genus muscle is a thin, ribbon-like muscle of the anterior knee. It is located on the anterior surface of the distal quarter of the femur. It is deep to, and many times embedded within the fibers of the vast us intermedius muscle.
- Proximal attachment: The anterolateral and anteromedial surfaces of the distal third of the femur
- Distal attachment: The suprapatellar bursa, synovial membrane and the joint capsule
- Action: Elevates or retracts the suprapatellar bursa during knee extension preventing mechanical impingement of the joint capsule between the patella and the femur
- Innervation: (L2, L3, L4) – femoral nerve (deep medial branch)
Role of Articularis Genus Muscle With Pain & Osteoarthritis
Due to its small size, the significance of the articularis genus muscle has previously had very little literature about it until this past decade in which a few research articles have surfaced that emphasize its importance with anterior knee pain and osteoarthritis. Woodley et al.2012 states “given its relationship to the anterior aspect of the knee joint and its association with the suprapatellar bursa, the articularis genus may be a neglected cause of undifferentiated anterior knee pain.”
Saito et, el 2016 discussed its importance with patients suffering from osteoarthritis. “Atrophic changes and dysfunctions in the AGM were observed in the OA (osteoarthritis) group with knee pain and limited knee ROM…..The AGM is an important therapeutic target in individuals with knee OA, whereby improvement in its contraction may contribute to improvement of symptoms.”
Articularis Genus Muscle Motor Point & Extra Point Jianxi
The exact motor entry point for this muscle is still under investigation by our team with our own cadaver dissections. However, according to Grob et el 2017, in their cadaver research, a medial branch off the femoral nerve inserts into the articularis genus. The exact innervation location of the AGM was not included in this article, but it did mention that after innervating the articularis genus muscle, the same nerve travelled distally to innervate the superior aspect of the synovial pouch and suprapatellar bursa. The superior aspect of the synovial pouch is located 2.5-3 cm. above the superior border of the patella (Gosling J.A. 2002). The muscle (fascicular) length of the articularis genus is on average 4.9 cm (Woodley, SJ. 2012). Therefore, the muscle belly of the articularis genus muscle is approximately 4-6 cm above the superior border of the patella or approximately 2.5-3 cun above the superior border of the patella (cun measurement is dependent on the size of the individual). This location, 3 cun above the superior border of the patella is the description for the extra point Jianxi.
Extra point Jianxi, translated as “Strengthen Knee” could potentially be the motor innervation of the articularis genus muscle. This extra point is located 3 cun directly above the center point of the superior border of the patella. This point received its name “Strengthen Muscle” most likely from evidential findings, therefore it is assumed that many practitioners before us have used this point for this reason. The indications for this point as used in the Shanghai University, China are paralysis of the knee and arthritis of the knee. (O’ Connor, J. 1981).
To needle this point, place the knee of the supine patient into flexion approximately 45˚- 60˚, the practitioner uses a 1.5-3 inch needle, angled with a slight inferior and oblique direction toward the femur. The needle sensation should spread into the anterior knee region.
References
- Grob, K. (2017). Surgical exposure of the hip joint and femur with a special emphasis on the architecture and function of the quadriceps muscle group and femoral blood supply.
- Gosling J.A. H.P. Whit more I. Willan P.L.T. Human anatomy: color atlas and text. 4th ed. Mosby, Toronto 2002: 269.
- O’Connor J, and Bensky D. Acupuncture: A Comprehensive Text. Shanghai College of Traditional Medicine. Seattle, WA: Eastland Press, 1981.
- Saito, A., Okada, K., Saito, I., Kinoshita, K., Seto, A., Takahashi, Y., … & Wakasa, M. (2016). Functional status of the articularis genus muscle in individuals with knee osteoarthritis. Journal of musculoskeletal & neuronal interactions, 16(4), 348.
- Woodley SJ, Latimer CP, Meikle GR, Stringer MD. Articularis genus: an anatomic and MRI study in cadavers. J Bone Joint Surg Am. 2012.
About the author(s):

Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.
About the author(s):
Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.