Medial Epicondylitis and the Heart Channel Sinews
Medial epicondylitis frequently occurs in activities that require repetitive shortening and lengthening (eccentric and concentric) contractions of the wrist flexors, which occur in activities of daily living, as well as in golf and throwing sports. Avid rock climbers, in whom this condition is referred to as climber’s elbow, are also susceptible to developing medial epicondylitis. Shortened or overused muscles pull on the tendinous attachment at the medial epicondyle and create pain and weakness. The diagnosis of medial epicondylitis is usually made from orthopedic evaluations that elicit pronounced tenderness at the medial epicondyle.
The three yin channel sinews (jingjin) of the arm are involved with medial epicondylitis. In relationship to the medial epicondyle, the relevant structures are:
- Flexor carpi radialis (LU jingjin)
- Pronator teres, finger flexors (P jingjin)
- Flexor carpi ulnaris (HT jingjin)
The type of activity determines which of these muscles will pull excessively on the medial epicondyle and, therefore, which is the likely contributor when a patient complains of pain at the medial epicondyle. Each of the above muscles should be considered in a differential diagnosis when assessing medial epicondylitis.
At the end of this blog, there are manual muscle tests (MMT) for each of these three muscles. Performing these MMTs will help determine which muscle is pulling excessively on the medial epicondyle. There is also a general orthopedic evaluative test for medial epicondylitis, as there are other conditions which have similar symptoms to medial epicondylitis. It is important to know what condition you are treating and then to determine which tissue imbalances are contributing to the fixed pain site. For more information on assessing and treating upper extremity injuries, sign up for Module 4 of the Sports Medicine Acupuncture Certification (SMAC) in 2019.
The HT sinew channel includes the flexor carpi ulnaris (FCU) muscle, which has the strongest and most direct pull on the medial epicondyle, making this a likely channel to include in assessment and treatment. The HT sinew channel shares the FCU with the SI sinew channel and is differentiated based on which muscles it links with (though its fascia) at its distal and proximal ends.
The FCU has two proximal attachments sites; a humeral head at the medial epicondyle, and an ulnar head at the proximal ulna and olecranon process. The HT sinew channel includes the humeral head of the FCU which attaches to the medial epicondyle. From the medial epicondyle, the HT sinew channel continues along the medial intermuscular septum, a thick fascial wall that travels up the medial arm to separate the biceps and the triceps. The SI sinew channel includes the FCU attachment located on more of the yang aspect of the elbow at the ulna and olecranon process. This head of the FCU shares fascia with the anconeus muscle and continues along with the triceps (Fig. 1).
Distally, the FCU also has multiple attachment sites. The FCU attaches to the pisiform bone where it has a very obvious connection with the adductor digiti minimi linking it with the SI sinew channel. It also has an attachment on the hook of the hamate and, via ligaments from here which link it to the base of the fifth metacarpal bone, connects with the third palmar interosseus muscle (located between metacarpal bones 4 and 5) and links with the HT sinew channel (Fig 1).
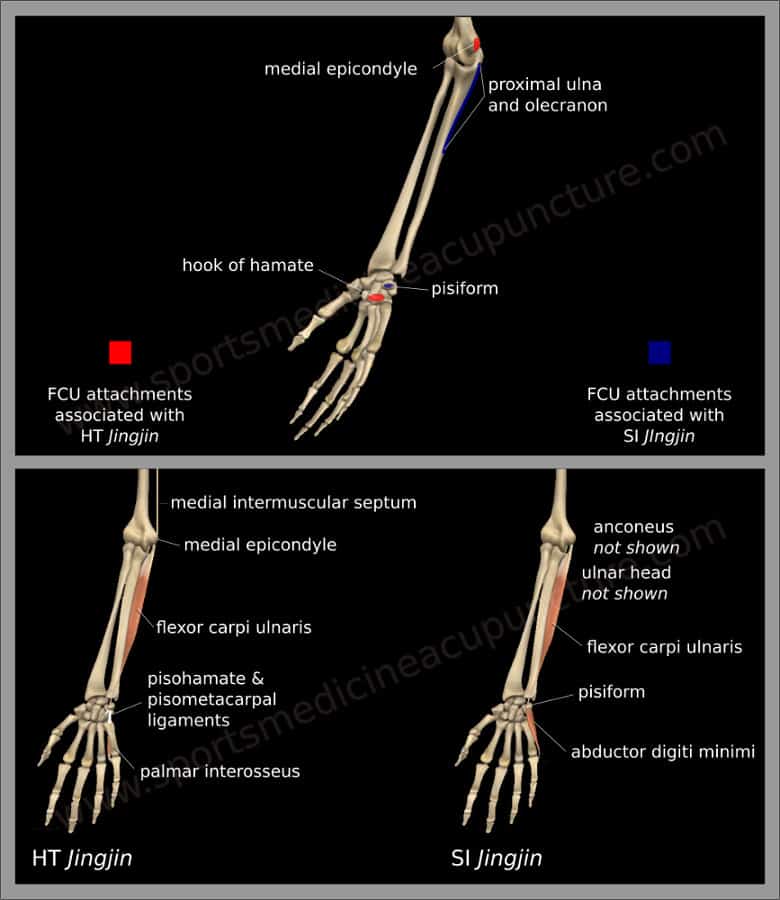
Figure 1: HT and SI sinew channels in the hand and forearm
The video for this article is from a recent Sports Medicine Acupuncture dissection, which highlights the HT sinew channel of the hand, forearm and elbow. There is an acupuncture needle inserted at HT 8 (shaofu) deep enough to affect the palmar interosseous muscle motor point. There is a needle inserted halfway between SI 3 (houxi) and SI 4 (wangu) into the abductor digiti minimi (ADM) motor point. A third needle is inserted the FCU motor point and a fourth needle, the control needle, is inserted into the medial epicondyle where pain is commonly found with epicondylitis.
The video is to demonstrate distal point selection when treating medial epicondylitis. We have concluded that the HT sinew channel may be a better channel to treat when the FCU is primarily involved in medial epicondylitis. The video shows that the force transmission from HT 8 was greater than the force transmission from the ADM motor point located on the SI jingjin. In other words, the myofascial connection of the palmar interosseus located at HT 8 can be used as an effective distal point to treat medial epicondylitis due to its communication along the HT sinew channel to the FCU attachment at the medial epicondyle.
The point of the video is not to suggest that one should turn the needle and pull as we are doing on the cadaver specimen, but to highlight the force transmission and to suggest that by removing obstructions along the channel, one should be able to regulate the amount of tension transmitted to the medial epicondyle proximally from a distal point. Simple needle techniques with the arrival of qi would regulate tension in the palmar interosseus and normalize tension in the HT sinew channel. Also, one can see that treating the FCU, especially at the motor point, will have an even more direct impact on the medial epicondyle.
The medial epicondyle is influenced not only by force transmission from below, but also by the pull along the HT jingjin located above the elbow. The medial intermuscular septum, the fascial wall between the biceps and triceps, is tensioned proximally by the pectoralis major and the subscapularis. These muscles tend to become overactive and lock-short, and, when observed in a static postural assessment, will show internal rotation of glenohumeral joint. Humeral internal rotation will offset the position of the medial epicondyle and result in an uneven pull of the muscles that attach to it. Treatment of one or both of these muscles to reduce their pull on the medial epicondyle through the medial intermuscular septum will increase therapeutic outcome.
There is a third muscle which can influence the medial intermuscular septum: the latissimus dorsi. This large muscle attaches very close to the pectoralis major and shares a strong fascial connection with it. Both the latissimus dorsi and the pectoralis major are part of the channel sinews of more than one channel. The pectoralis major is part of the continuous myofascial plane of the HT sinew channel, as described above (palmar interosseus, FCU, medial intermuscular septum, pectoralis major and subscapularis). The latissimus dorsi and pectoralis major (as a fascial unit) are also part of the channel sinews of both the UB and the GB channel sinews. How they interact with the forces from the pelvis to the shoulder girdle is a discussion for another time. In regard to medial epicondylitis, it is useful to consider treating the latissimus dorsi. Also, since the latissimus dorsi connects the shoulder girdle to the pelvic girdle, balancing the pelvis will integrate any work you do above (the shoulder girdle and upper extremities) with below (the pelvic girdle). We spend a considerable amount of time assessing and treating pelvic imbalance in Module 2 in the Sports Medicine Acupuncture Certification (SMAC).
So far, we have suggested possible distal points (on the HT channel), adjacent points (FCU MP), and point selection below to treat above. There are two further suggestions for a balanced acupuncture treatment. First, select points to regulate any zangfu disharmony, and any disharmony of Qi, Blood or Body Fluids. Second, treat locally at the fixed pain site, assuming that this isn’t an acute condition which might contraindicate local treatment. See a description of the local technique in the soon-to-be-released book Sports Medicine Acupuncture: An Integrated Approach Combining Sports Medicine and Traditional Chinese Medicine, by Matt Callison, or attend classes with the Sports Medicine Acupuncture Certification.

Figure 2. Flexor carpi ulnaris manual muscle test
Flexor Carpi Ulnaris Manual Muscle Test
- The seated or supine patient places their elbow into 30˚ of flexion with their wrist supinated with slight flexion and ulnar deviation.
- The practitioner’s stabilizing hand supports the underside of the forearm. The practitioner’s other hand covers the patient’s palm with pressure directed onto the hypothenar eminence, specifically the palmar side of SI 3 (houxi) and SI 4 (wangu) (Fig. 2).
- The line of drive is in the direction of wrist extension, toward the radial side.
Note: Watch for finger flexion as the patient may try to recruit other flexor muscles to compensate for a weak flexor carpi ulnaris.

Figure 3. Flexor carpi radialis manual muscle test
Flexor Carpi Radialis Manual Muscle Test
- The seated or supine patient places their forearm into a neutral position and their wrist into radial deviation with slight flexion.
- The patient’s hand and wrist are supported by the practitioner’s hand. The practitioner places 2-3 fingers of their other hand over the patient’s thenar eminence in the area of LU 10 (yuji).
- The line of drive is into wrist extension toward the ulnar side (Fig. 3).
Pronator Teres Manual Muscle Test

Figure 4. Pronator teres manual muscle test
- With the patient in a seated or supine position, adduct the shoulder and flex the elbow to 20˚-45˚ with the forearm held in a pronated position so that P 8 (laogong) faces down.
- The practitioner’s stabilizing hand supports the elbow while the driving hand covers the area of P7 (daling) and LU 10 (yuji) (Fig. 4).
- The line of drive is to create supination, which will cause laogong to face superiorly.
Note: Watch for elbow flexion as the patient recruits the biceps brachii.

Figure 5. Extending the fingers increases the stretch of the wrist flexor
Medial Epicondylitis Test
This test assesses for pain at the common flexor attachment on the medial epicondyle, indicating the possibility of medial epicondylitis.
- Place the patient’s elbow and wrist into extension with the forearm supinated.
- The practitioner supports the patient’s elbow and increases the stretch by further extending the fingers (Fig. 5).
- A positive test produces pain at the medial epicondyle. The practitioner will need to palpate the common flexor attachment to confirm that the pain is at the medial epicondyle.
To learn more about AcuSport Education’s educational offerings, go here:
About the author(s):

Brian Lau, AP, C.SMA is has been on the faculty of the Sports Medicine Acupuncture Certification since 2014, and also teaches foundation courses with AcuSport Education. Brian lives and practices in Tampa, FL where he owns and operates Ideal Balance: Center for Sports Medicine Acupuncture (www.ideal-balance.net). He blogs on anatomy and TCM at www.sinewchannels.com.

Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.
About the author(s):
Brian Lau, AP, C.SMA is has been on the faculty of the Sports Medicine Acupuncture Certification since 2014, and also teaches foundation courses with AcuSport Education. Brian lives and practices in Tampa, FL where he owns and operates Ideal Balance: Center for Sports Medicine Acupuncture (www.ideal-balance.net). He blogs on anatomy and TCM at www.sinewchannels.com.
Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.