Assessment & Treatment of the Channel Sinews for Posterior & Medial Knee Pain
There are many injuries that affect the Urinary Bladder and Kidney channel sinews (jingjin). Having a detailed understanding of the myofascial anatomy associated with these channels is especially important to the practitioner practicing or studying Sports Medicine Acupuncture®, or to any practitioner who applies orthopedic or sports medicine principles in their acupuncture treatments. Below is a brief summary of posterior and medial knee pain associated with the UB and the KID jingjin.
To be clear, there are many knee injuries that need to be properly assessed and these injuries can involve multiple channels. The goal of this post is not to expand on the assessment and treatment of all of these injuries, but to give some brief information regarding a few injuries which are associated with the UB and KID jingjin, and to describe how these injuries relate to imbalances within the jingjin. Understanding the anatomy associated with the jingjin helps integrate orthopedic evaluation with the Chinese medical channel system and can serve as a link when applying sports medicine principles in TCM practice.
If you would like to learn more about assessment and local treatment of these injuries, the 10th cycle of SMAC (Sports Medicine Acupuncture Certification) will start in Bloomfield, New Jersey in October 2019. Alternatively, you can sign up for one of the 2-day SMA Foundational courses. Click here for the calendar of classes.
Also, below is a brief video associated with the layered anatomy of these channel sinews. You may want to review this video before or after reading the post.
(Click on the PLAY button on the video)
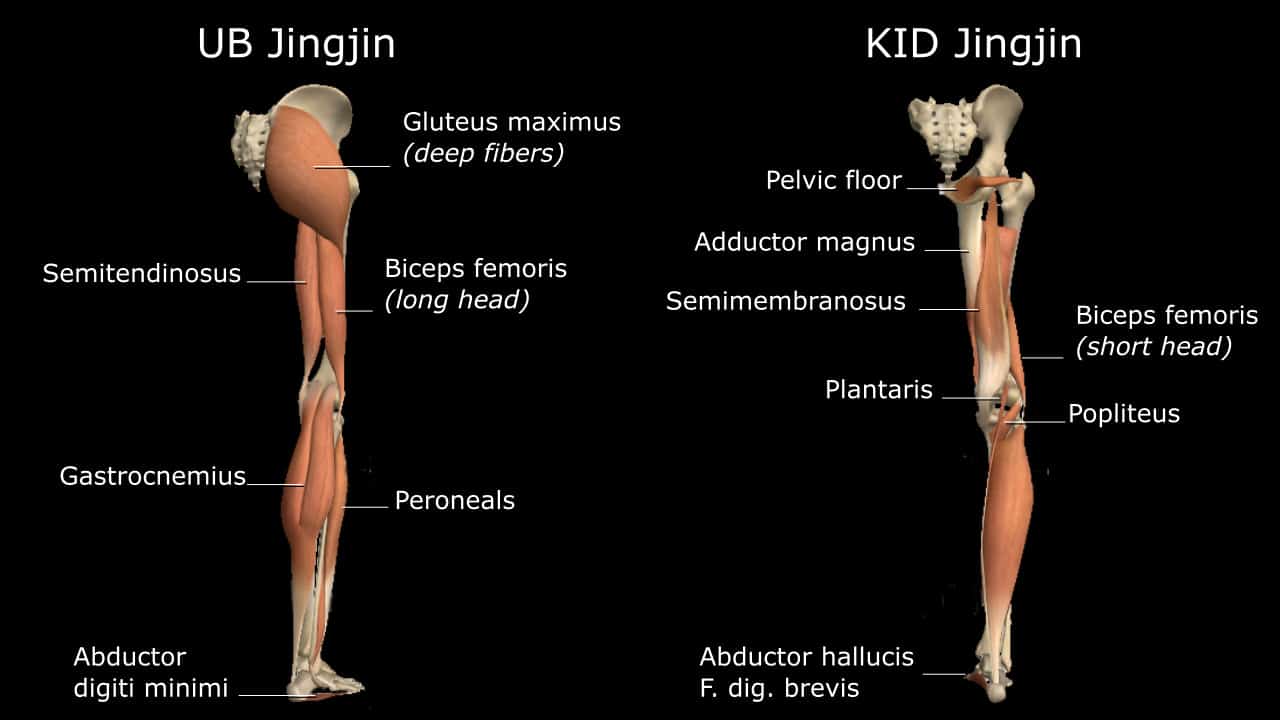
Three common injuries associated with the UB and the KID jingjin are upper gastrocnemius strain, hamstring tenosynovitis and medial collateral ligament strain. These present with posterior or medial knee pain, depending on the injury. Again, this post is not focused on assessment and treatment of these injuries, but on understanding the myofascial connections associated with the involved structures, which allows the acupuncturist to choose additional points for treatment beyond just working with the local injury.
To explain further and in context to this blog post, the Urinary Bladder jingjin is involved with upper gastrocnemius strain and hamstring tenosynovitis. Both of these groups of muscles are part of the UB jingjin. Actually, the hamstrings are a bit more complicated, and the video will detail this in more depth. For the purpose of this blog post, we will look at these injuries as being associated with the UB jingjin. These two major muscle groups, when imbalanced, can be two major generators of posterior knee pain. Once an accurate diagnosis of either of these two injuries is confirmed, the practitioner can palpate the structures, assessing for pain levels on a scale of 1-10. The practitioner can use Acupuncture as an Assessment on key points on the affected channels such as channel points or motor points (MPs) of muscles along the UB channel to help reduce pain with palpation. These points include but are not limited to the adductor digiti minimi MP (UB 64), the xi-cleft point of the UB channel (UB 63), and/or the piriformis motor point due to particular imbalances in the jingjin due to postural imbalances that can affect the knee.
With medial knee pain, the MCL has a very strong fascial connection with the adductor magnus (they are on the same plane of tissue) and with the distal semimembranosus (this muscle has a fascia expansion which connects with the MCL). Each of these tissues belongs to the KID jingjin, and Including the adductor magnus and semimembranosus muscle MPs will assist in relieving pain and speeding recovery of MCL strain.
 The practitioner should start with ortho exams such as valgus stress test and Apley’s distraction test combined with a thorough history exploring mechanism of injury. Then Acupuncture as Assessment can be performed in the same way as described above. The practitioner palpates the MCL along its length to locate the site of greatest pain and injury. Ask the patient to state the pain level on a scale of 1-10. Needle the adductor magnus MP obtaining deqi, and then return to the fixed pain site on the MCL and again have the patient state the pain level. You can also include the semimembranosus MP into this assessment.
The practitioner should start with ortho exams such as valgus stress test and Apley’s distraction test combined with a thorough history exploring mechanism of injury. Then Acupuncture as Assessment can be performed in the same way as described above. The practitioner palpates the MCL along its length to locate the site of greatest pain and injury. Ask the patient to state the pain level on a scale of 1-10. Needle the adductor magnus MP obtaining deqi, and then return to the fixed pain site on the MCL and again have the patient state the pain level. You can also include the semimembranosus MP into this assessment.
Acupuncture to these MPs reduce pain by about 50%. Since these are such consistent pain reducing points for MCL pain, it would be useful to reinsert these points when you are performing your full treatment. This would include local treatment to the MCL (in SMAC, we teach an incredible technique developed by Matt Callison to return integrity to an injured MCL), distal points (KID 5 is a very useful point to move qi in the Kidney channel), and other points based on your postural assessment, orthopedic assessment, functional tests and TCM assessment.
As acupuncturists know, it is sometimes the case that treatment of the channel associated with the injury and the TCM Pattern associated with the patient yields excellent results, but that sometimes results are not lasting. This might be the case with posterior knee pain. The suggestions described in this post, combined with good local treatment should yield results, but the pain might be persistent if you only treat the channel where the pain is. For instance, sometimes the Kidney channel needs also to be addressed when there is pain in the posterior knee involving structures of the UB jingjin. These channels are internally-externally related and interact with each other energetically, of course, but also mechanically.
 For instance, damage to the ligaments of the knee, especially the PCL and posterior capsule of the knee, will create instability of the knee, which calls on greater involvement of the gastrocnemius and hamstrings for stability, creating a greater likelihood of pain and injury to these overused structures. We teach needling for the PCL in SMAC, but treatment of the MP of the semimembranosus is an easy way to indirectly reach these ligamentous structures of the knee. This is because the distal semimembranosus, sometimes referred to as the pes anserine profundus, has a complex relationship to posterior knee stability and proprioception, as it is closely linked with the posterior capsule complex of the knee. The semimembranosus and the posterior capsule complex of the knee is part of the KID jingjin, so treatment of posterior knee instability through the KID jingjin can be necessary with pain in the UB jingjin.
For instance, damage to the ligaments of the knee, especially the PCL and posterior capsule of the knee, will create instability of the knee, which calls on greater involvement of the gastrocnemius and hamstrings for stability, creating a greater likelihood of pain and injury to these overused structures. We teach needling for the PCL in SMAC, but treatment of the MP of the semimembranosus is an easy way to indirectly reach these ligamentous structures of the knee. This is because the distal semimembranosus, sometimes referred to as the pes anserine profundus, has a complex relationship to posterior knee stability and proprioception, as it is closely linked with the posterior capsule complex of the knee. The semimembranosus and the posterior capsule complex of the knee is part of the KID jingjin, so treatment of posterior knee instability through the KID jingjin can be necessary with pain in the UB jingjin.
Proper assessment is essential when combining sports medicine principles with TCM. Orthopedic evaluation along with a TCM pattern differentiation should be the starting place. Understanding the anatomy of the channel sinews (jingjin) can serve as a link and will vastly improve results when treating patients with sports injuries and orthopedic conditions, such as posterior and medial knee pain.
To learn more about AcuSport Education’s educational offerings, go here:
About the author(s):
There are many injuries that affect the Urinary Bladder and Kidney channel sinews (jingjin). Having a detailed understanding of the myofascial anatomy associated with these channels is especially important to the practitioner practicing or studying Sports Medicine Acupuncture®, or to any practitioner who applies orthopedic or sports medicine principles in their acupuncture treatments. Below is a brief summary of posterior and medial knee pain associated with the UB and the KID jingjin.
To be clear, there are many knee injuries that need to be properly assessed and these injuries can involve multiple channels. The goal of this post is not to expand on the assessment and treatment of all of these injuries, but to give some brief information regarding a few injuries which are associated with the UB and KID jingjin, and to describe how these injuries relate to imbalances within the jingjin. Understanding the anatomy associated with the jingjin helps integrate orthopedic evaluation with the Chinese medical channel system and can serve as a link when applying sports medicine principles in TCM practice.
If you would like to learn more about assessment and local treatment of these injuries, the 10th cycle of SMAC (Sports Medicine Acupuncture Certification) will start in Bloomfield, New Jersey in October 2019. Alternatively, you can sign up for one of the 2-day SMA Foundational courses. Click here for the calendar of classes.
Also, below is a brief video associated with the layered anatomy of these channel sinews. You may want to review this video before or after reading the post.
(Click on the PLAY button on the video)
Three common injuries associated with the UB and the KID jingjin are upper gastrocnemius strain, hamstring tenosynovitis and medial collateral ligament strain. These present with posterior or medial knee pain, depending on the injury. Again, this post is not focused on assessment and treatment of these injuries, but on understanding the myofascial connections associated with the involved structures, which allows the acupuncturist to choose additional points for treatment beyond just working with the local injury.
To explain further and in context to this blog post, the Urinary Bladder jingjin is involved with upper gastrocnemius strain and hamstring tenosynovitis. Both of these groups of muscles are part of the UB jingjin. Actually, the hamstrings are a bit more complicated, and the video will detail this in more depth. For the purpose of this blog post, we will look at these injuries as being associated with the UB jingjin. These two major muscle groups, when imbalanced, can be two major generators of posterior knee pain. Once an accurate diagnosis of either of these two injuries is confirmed, the practitioner can palpate the structures, assessing for pain levels on a scale of 1-10. The practitioner can use Acupuncture as an Assessment on key points on the affected channels such as channel points or motor points (MPs) of muscles along the UB channel to help reduce pain with palpation. These points include but are not limited to the adductor digiti minimi MP (UB 64), the xi-cleft point of the UB channel (UB 63), and/or the piriformis motor point due to particular imbalances in the jingjin due to postural imbalances that can affect the knee.
With medial knee pain, the MCL has a very strong fascial connection with the adductor magnus (they are on the same plane of tissue) and with the distal semimembranosus (this muscle has a fascia expansion which connects with the MCL). Each of these tissues belongs to the KID jingjin, and Including the adductor magnus and semimembranosus muscle MPs will assist in relieving pain and speeding recovery of MCL strain.
The practitioner should start with ortho exams such as valgus stress test and Apley’s distraction test combined with a thorough history exploring mechanism of injury. Then Acupuncture as Assessment can be performed in the same way as described above. The practitioner palpates the MCL along its length to locate the site of greatest pain and injury. Ask the patient to state the pain level on a scale of 1-10. Needle the adductor magnus MP obtaining deqi, and then return to the fixed pain site on the MCL and again have the patient state the pain level. You can also include the semimembranosus MP into this assessment.
Acupuncture to these MPs reduce pain by about 50%. Since these are such consistent pain reducing points for MCL pain, it would be useful to reinsert these points when you are performing your full treatment. This would include local treatment to the MCL (in SMAC, we teach an incredible technique developed by Matt Callison to return integrity to an injured MCL), distal points (KID 5 is a very useful point to move qi in the Kidney channel), and other points based on your postural assessment, orthopedic assessment, functional tests and TCM assessment.
As acupuncturists know, it is sometimes the case that treatment of the channel associated with the injury and the TCM Pattern associated with the patient yields excellent results, but that sometimes results are not lasting. This might be the case with posterior knee pain. The suggestions described in this post, combined with good local treatment should yield results, but the pain might be persistent if you only treat the channel where the pain is. For instance, sometimes the Kidney channel needs also to be addressed when there is pain in the posterior knee involving structures of the UB jingjin. These channels are internally-externally related and interact with each other energetically, of course, but also mechanically.
For instance, damage to the ligaments of the knee, especially the PCL and posterior capsule of the knee, will create instability of the knee, which calls on greater involvement of the gastrocnemius and hamstrings for stability, creating a greater likelihood of pain and injury to these overused structures. We teach needling for the PCL in SMAC, but treatment of the MP of the semimembranosus is an easy way to indirectly reach these ligamentous structures of the knee. This is because the distal semimembranosus, sometimes referred to as the pes anserine profundus, has a complex relationship to posterior knee stability and proprioception, as it is closely linked with the posterior capsule complex of the knee. The semimembranosus and the posterior capsule complex of the knee is part of the KID jingjin, so treatment of posterior knee instability through the KID jingjin can be necessary with pain in the UB jingjin.
Proper assessment is essential when combining sports medicine principles with TCM. Orthopedic evaluation along with a TCM pattern differentiation should be the starting place. Understanding the anatomy of the channel sinews (jingjin) can serve as a link and will vastly improve results when treating patients with sports injuries and orthopedic conditions, such as posterior and medial knee pain.
To learn more about AcuSport Education's educational offerings, go here:
About the author(s):
There are many injuries that affect the Urinary Bladder and Kidney channel sinews (jingjin). Having a detailed understanding of the myofascial anatomy associated with these channels is especially important to the practitioner practicing or studying Sports Medicine Acupuncture®, or to any practitioner who applies orthopedic or sports medicine principles in their acupuncture treatments. Below is a brief summary of posterior and medial knee pain associated with the UB and the KID jingjin.
To be clear, there are many knee injuries that need to be properly assessed and these injuries can involve multiple channels. The goal of this post is not to expand on the assessment and treatment of all of these injuries, but to give some brief information regarding a few injuries which are associated with the UB and KID jingjin, and to describe how these injuries relate to imbalances within the jingjin. Understanding the anatomy associated with the jingjin helps integrate orthopedic evaluation with the Chinese medical channel system and can serve as a link when applying sports medicine principles in TCM practice.
If you would like to learn more about assessment and local treatment of these injuries, the 10th cycle of SMAC (Sports Medicine Acupuncture Certification) will start in Bloomfield, New Jersey in October 2019. Alternatively, you can sign up for one of the 2-day SMA Foundational courses. Click here for the calendar of classes.
Also, below is a brief video associated with the layered anatomy of these channel sinews. You may want to review this video before or after reading the post.
(Click on the PLAY button on the video)
Three common injuries associated with the UB and the KID jingjin are upper gastrocnemius strain, hamstring tenosynovitis and medial collateral ligament strain. These present with posterior or medial knee pain, depending on the injury. Again, this post is not focused on assessment and treatment of these injuries, but on understanding the myofascial connections associated with the involved structures, which allows the acupuncturist to choose additional points for treatment beyond just working with the local injury.
To explain further and in context to this blog post, the Urinary Bladder jingjin is involved with upper gastrocnemius strain and hamstring tenosynovitis. Both of these groups of muscles are part of the UB jingjin. Actually, the hamstrings are a bit more complicated, and the video will detail this in more depth. For the purpose of this blog post, we will look at these injuries as being associated with the UB jingjin. These two major muscle groups, when imbalanced, can be two major generators of posterior knee pain. Once an accurate diagnosis of either of these two injuries is confirmed, the practitioner can palpate the structures, assessing for pain levels on a scale of 1-10. The practitioner can use Acupuncture as an Assessment on key points on the affected channels such as channel points or motor points (MPs) of muscles along the UB channel to help reduce pain with palpation. These points include but are not limited to the adductor digiti minimi MP (UB 64), the xi-cleft point of the UB channel (UB 63), and/or the piriformis motor point due to particular imbalances in the jingjin due to postural imbalances that can affect the knee.
With medial knee pain, the MCL has a very strong fascial connection with the adductor magnus (they are on the same plane of tissue) and with the distal semimembranosus (this muscle has a fascia expansion which connects with the MCL). Each of these tissues belongs to the KID jingjin, and Including the adductor magnus and semimembranosus muscle MPs will assist in relieving pain and speeding recovery of MCL strain.
The practitioner should start with ortho exams such as valgus stress test and Apley’s distraction test combined with a thorough history exploring mechanism of injury. Then Acupuncture as Assessment can be performed in the same way as described above. The practitioner palpates the MCL along its length to locate the site of greatest pain and injury. Ask the patient to state the pain level on a scale of 1-10. Needle the adductor magnus MP obtaining deqi, and then return to the fixed pain site on the MCL and again have the patient state the pain level. You can also include the semimembranosus MP into this assessment.
Acupuncture to these MPs reduce pain by about 50%. Since these are such consistent pain reducing points for MCL pain, it would be useful to reinsert these points when you are performing your full treatment. This would include local treatment to the MCL (in SMAC, we teach an incredible technique developed by Matt Callison to return integrity to an injured MCL), distal points (KID 5 is a very useful point to move qi in the Kidney channel), and other points based on your postural assessment, orthopedic assessment, functional tests and TCM assessment.
As acupuncturists know, it is sometimes the case that treatment of the channel associated with the injury and the TCM Pattern associated with the patient yields excellent results, but that sometimes results are not lasting. This might be the case with posterior knee pain. The suggestions described in this post, combined with good local treatment should yield results, but the pain might be persistent if you only treat the channel where the pain is. For instance, sometimes the Kidney channel needs also to be addressed when there is pain in the posterior knee involving structures of the UB jingjin. These channels are internally-externally related and interact with each other energetically, of course, but also mechanically.
For instance, damage to the ligaments of the knee, especially the PCL and posterior capsule of the knee, will create instability of the knee, which calls on greater involvement of the gastrocnemius and hamstrings for stability, creating a greater likelihood of pain and injury to these overused structures. We teach needling for the PCL in SMAC, but treatment of the MP of the semimembranosus is an easy way to indirectly reach these ligamentous structures of the knee. This is because the distal semimembranosus, sometimes referred to as the pes anserine profundus, has a complex relationship to posterior knee stability and proprioception, as it is closely linked with the posterior capsule complex of the knee. The semimembranosus and the posterior capsule complex of the knee is part of the KID jingjin, so treatment of posterior knee instability through the KID jingjin can be necessary with pain in the UB jingjin.
Proper assessment is essential when combining sports medicine principles with TCM. Orthopedic evaluation along with a TCM pattern differentiation should be the starting place. Understanding the anatomy of the channel sinews (jingjin) can serve as a link and will vastly improve results when treating patients with sports injuries and orthopedic conditions, such as posterior and medial knee pain.
To learn more about AcuSport Education's educational offerings, go here: