Sacroiliac Joint Pain and the Pelvic Floor: An Approach for the Acupuncturist

Sacroiliac joint pain is a common injury and is often the result of dysfunctional motion in the sacroiliac joint (SIJ). Studies have documented that motion occurs at the SIJ; therefore, hypomobility or hypermobility of the sacroiliac joint can lead to pain (Kiapour, A., 2020). Increased or decreased movement in the SIJ is primarily stemming from pelvic girdle imbalances. When injury occurs, the patient will often feel localized pain anterior and medial to the PSIS, in addition to associated pain reported in the gluteal region, anterior groin or a discomfort described as “feeling internal.”
Common Causes of Sacroiliac Joint Pain
Sacroiliac joint pain is most frequently due to pelvic and myofascial imbalances combined with repetitive activities that eventually exceed the limit of what the joint and ligaments can withstand.
The patient may report pain that started with a small incident, such as picking up a ball from the court or bending over to put something into the back seat of a car or pain that slowly occurred during an activity, only to become worse after a period of time.
It’s difficult to definitively state specific pelvic imbalances that are consistent with sacroiliac joint pain; however, it is common to find some combination of an elevated ilium, a pelvic tilt and/or a pelvic rotation. These pelvic imbalances typically coincide with myofascial imbalances in some combination of the iliopsoas, gluteus maximus, quadratus lumborum, piriformis, biceps femoris, multifidus and abdominal muscles, any of which can alter the normal movement of the pelvis on the sacrum. (Neme, J. R. 2022).
Not commonly mentioned or discussed in clinical treatment approaches for pelvic imbalances is using and understanding the pelvic floor musculature and its role in postural support.
Sacroiliac Joint Pain & Pelvic Floor Musculature
There is increasing evidence for the link between sacroiliac joint pain and dysfunction and the pelvic floor musculature (Dufour, S., 2018).
Before going further, let’s define the pelvic floor for this article. The levator ani is the primary aspect of the pelvic floor and supports and raises the pelvic visceral structures for proper sexual functioning, defecation and urination. It is a broad, thin muscle, situated on both sides of the pelvis. It is formed from three muscle components: the pubococcygeus, the iliococcygeus and the puborectalis. The levator ani is supported by three muscles: the obturator internus that suspends the levator ani, the coccygeus that firmly protects and posteriorly stabilizes the levator ani and the piriformis, which many researchers include as part of the pelvic floor due to its supportive role similar to the coccygeus.

Figure 1 Levator ani muscles are in green and other pelvic floor muscles include the the obturator internus, coccygeus and piriformis muscles in red.
There is significant controversy amongst anatomists with regards to the nomenclature and which muscles do and do not belong to the pelvic floor. For the purposes of clarity, in this article, all muscle shown in Fig. 1 will be referred to as the pelvic floor.
With pelvic imbalances, the pelvic floor, which normally acts as an integrated unit, adapts to the pelvic tilting and/or torsion position. As a result, pelvic floor muscles have difficulty in coordinating their normal role of relaxation and activation. Typical with muscle imbalances, when one component is compromised, opposing muscles adapt and the normal force-tension relationship is altered, resulting in dysfunction, aberrant proprioceptive neural signaling and pain. Increased tone and shortening of pelvic floor muscle fibers increases tension and eventually develops into contracture and adhesions. In a cadaver study, the researchers simulated tension in the pelvic floor muscles that increased SIJ immobility and altered its normal function. (Pool-Goudzwaard)
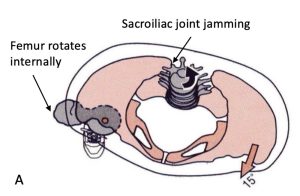
Figure 2. A. The right femur in compensation for a pelvic rotation to the right during weight bearing. Image from Neumann DA. Kinesiology of the Musculoskeletal System. B. Posterior view of right obturator internus and motor entry point location.
Women suffer from sacroiliac joint pain more than men and is most likely due to the different angulation of the pelvic girdle and SIJ between the sexes that predisposes the joint to excessive motion and ligamentous strain. Gyang, A. et al. (2013) found that 22% of women with pelvic floor dysfunction (PFD) also have low back pain including sacroiliac joint pain. (Kiapour, A., 2020). In addition, PFD has been found to affect up to 1/3 of women in the United States. (Lawrence, J. M., 2008).
Pelvic floor musculature commonly involved in sacroiliac joint pain are the piriformis and coccygeus muscles. These muscles directly attach to the sacrum and act as a “guy-wire” for sacral stabilization (Fig. 1 & 3). In the author’s opinion, these muscles and their associated myofascial channels (piriformis, UB, coccygeus, KID) should be prioritized in treatment of sacroiliac joint pain and pelvic floor dysfunction (PFD). In addition, the obturator internus , a primary external rotator of the hip, suspends and balances the levator ani on left and right sides via the highly proprioceptive arcus tendinous fascia. When pelvic rotation is involved with SIJ pain, the obturator internus muscles are imbalanced due to compensatory femoral rotation. For example, pelvic rotation to the right will bring the right femur into a compensatory internal rotation and lengthen parts of this muscle, which is predisposition to potential injury to the hip and levator ani. (Fig. 2)
Sacrotuberous Ligament & Sacroiliac Joint Pain

Figure 3. Top image: Sacrotuberous ligament covers the coccygeus muscle and is an important anatomical landmark. Bottom image: Perpendicular palpation to the middle region of the sacrotuberous ligament will often identify tender ashi points.
A common finding in patients with sacroiliac joint pain is increased tension and shortening of the biceps femoris muscle assessed through a hamstring length test. The biceps femoris has a direct effect on the stability of the SIJ via its fascial/tendinous attachments to the sacrotuberous ligament. (Ashby, K., 2022). Anatomically, the sacrotuberous ligament attaches from the ischial tuberosity to the lower aspect of the sacrum in the region of UB 34 (xialiao) and is the posterior support for the coccygeus muscle, an important pelvic floor muscle involved in sacroiliac joint pain and dysfunction. Increased tension in the sacrotuberous ligament hinders sacral motion and can result in pelvic floor muscle imbalances and low back pain including sacroiliac joint pain. (Sasaki, T., 2021).
Figure 3 shows palpation of the sacrotuberous ligament in preparation for acupuncture needle technique. The sacrotuberous ligament and biceps femoris are part of the UB primary (jingluo) and channel sinews (jingjin) therefore adjacent and distal points from these channels would be combined with local needling.
Common Postures Observed in These Conditions

Figure 4. An anterior tilt and anterior hip shift posture common with sacroiliac joint pain and pelvic floor dysfunction.
Common postures seen in patients with these conditions are an anterior tilt, an elevated ilium and/or an anterior hip shift. Figure 4 shows a lateral view of a patient with sacroiliac joint pain and pelvic floor dysfunction. The patient can be observed to have an anterior pelvic tilt (yellow line) with an anterior hip shift.
Anterior hip shift, as the name implies, is a posture where the greater trochanter is anterior to GB 40 (lower yellow dot) and the acromion at LI 15 (upper yellow dot). This posture adds excessive stress on the normal length-tension relationship of pelvic floor musculature and sacroiliac joints. Treating these postural deviations and their myofascial channel imbalances is imperative for successful and long-lasting results in not only sacroiliac joint pain and pelvic floor dysfunction, but also for lower jiao organ pathology, such as bladder pain and irritable bowel syndrome.
It is important to note, from the author’s research and presentations, this particular posture (Fig. 4) will have deep Kidney pulses and a qi and blood deficient tongue appearance. Other Kidney signs and symptoms will probably be present.

As we have learned in TCM theory, affecting the external environment will directly affect the internal environment. In the Sports Medicine Acupuncture Certification (SMAC) Program, we excel in the education of assessment and treatment of musculoskeletal pain and dysfunction using acupuncture, therapeutic myofascial techniques and corrective exercise.
Module II: The Low Back, Hip and Groin
- January 17-19, 2024 — Postural Imbalances and Acupuncture Protocols (San Diego, CA)
- January 20-21, 204 — Myofascial Techniques and Therapeutic Exercise Protocols (San Diego, CA)
- April 17-21, 2024 — Assessment and Treat of Injury (Bloomfield, New Jersey)
- May 1-5, 2024 — Assessment and Treat of Injury (San Diego, CA)
In Module II, students will learn how to:
- Assess and normalize postural dysfunctions that have contributed to injury, not only for musculoskeletal pain but also pelvic floor pain and dysfunction and organ related pathologies.
- Learn advanced needle techniques for over 28 different injuries and needle technique over 45 different muscles including accessible pelvic floor musculature.

The SMAC courses can be taken individually and are based in traditional Chinese medicine and discussed through the lens of Sports Medicine and western biomedicine.
Related Topics:
References:
Dufour, S., Vandyken, B., Forget, M. J., & Vandyken, C. (2018). Association between lumbopelvic pain and pelvic floor dysfunction in women: A cross sectional study. Musculoskeletal Science and Practice, 34, 47-53.
Kiapour, A., Joukar, A., Elgafy, H., Erbulut, D. U., Agarwal, A. K., & Goel, V. K. (2020). Biomechanics of the sacroiliac joint: anatomy, function, biomechanics, sexual dimorphism, and causes of pain. International journal of spine surgery, 14(s1), S3-S13.
Gyang, A., Hartman, M., & Lamvu, G. (2013). Musculoskeletal causes of chronic pelvic pain: what a gynecologist should know. Obstetrics & Gynecology, 121(3), 645-650.
Lawrence, J. M., Lukacz, E. S., Nager, C. W., Hsu, J. W. Y., & Luber, K. M. (2008). Prevalence and co-occurrence of pelvic floor disorders in community-dwelling women. Obstetrics & Gynecology, 111(3), 678-685.
Neme, J. R. (2022). Balancing Act: Muscle imbalance effects on musculoskeletal injuries. Missouri Medicine, 119(3), 225.
Pool-Goudzwaard, A., van Dijke, G. H., van Gurp, M., Mulder, P., Snijders, C., & Stoeckart, R. (2004). Contribution of pelvic floor muscles to stiffness of the pelvic ring. Clinical Biomechanics, 19(6), 564-571.
Sasaki, T., Kurosawa, D., Murakami, E., & Watanabe, T. (2021). Physical therapeutic options for residual sacrotuberous ligament pain after treatment of sacroiliac joint dysfunction. Journal of physical therapy science, 33(9), 646-652.).
About the author(s):

Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.
About the author(s):
Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.