Telemedicine Guide: A Low Back Pain Case Study

This article and the accompanying video are meant to share our experience with developing, designing and working through the logistical issues of a telemedicine consultation. Our goal is to help practitioners learn a different way to help their patients during these challenging and ever-changing times of COVID-19.
Initially, the information in this article was supposed to be presented in a live webinar produced by Matt Callison and Brian Lau. This content was designed for students and graduates of the Sports Medicine Acupuncture Certification (SMAC) program and it was intended to be a review of the recently completed Module II: Low Back, Hip and Groin (completed just before the COVID-19 shutdown). Our plan for the live webinar was to provide examples of how to apply some of the principles taught in SMAC through a telemedicine format. The trial run version of the video was recorded over two days as we learned and experimented with using the different features of a digital platform, as well as the logistics of using different devices and camera angles.
Helping Patients with Telemedicine
The surge in demand for telemedicine consultations, coupled with the fact that most practitioners haven’t had much experience in long distance consultation, prompted us to decide to release the trial run video as a learning tool, so practitioners could see our process. In this video, the viewer will see Matt and Brian making decisions on how to guide a patient through an assessment for her low back pain in order to build a self-applied treatment plan and protocol.
Keep in mind, the creation of this video recording was a trial run project and the patient is a SMAC graduate/faculty and, therefore, Matt and Brian did not always give clear directions on patient positioning as they might have done with a patient with less training. Also, there is a lot of open dialogue, which shows some of the thought processes that Matt and Brian were undergoing as they experimented with what worked and what didn’t for a digital telemedicine format.
The surge in demand for telemedicine consultations prompted us to decide to release the trial run video as a learning tool, so practitioners could see our process.
We will start this telemedicine case study, which is presented in an outline form, with some logistical issues that we came across that can hopefully help the practitioner to create a good environment for assessing and recording their patients performing orthopedic examinations and postural exams. This is followed by a discussion of the telemedicine case study and finally, a prescription for home care including acupressure points and rehabilitative exercises.
Telemedicine Considerations
Patient Consent Forms
- Contact your State Acupuncture Board for more information on guidelines and regulations regarding telemedicine consultations.
Preparing the Space and Distancing the Camera
- Ask the patient to prepare the space, preferably with a blank wall in the background (this is best for video quality). From our experience, to get a full-body view on a tablet or laptop, the patient should be positioned about 7-8 feet away from the camera. Of course, this will change depending on the height of the patient and the equipment they are using. Having enough space is important, but not mandatory. Make the best of the space that is provided. The goal is for the practitioner to have a clear view of the patient, as well as to watch them perform static and functional assessments.
- We asked the patient to perform the ortho and postural exams in standing, seated and supine positions.
- If possible, ask the patient to place a 3 foot strip of duct tape perpendicular to the wall (at a 90˚ angle). This will help to keep the patient in the same location when the practitioner is examining both left and right sides from a lateral view. It will also help to guide the patient with feet placement when the practitioner is viewing the anterior and posterior views.
Getting the Best Camera Angle
- This can be difficult and it depends on which device the patient is using for the telemedicine appointment. We found that a tablet was very useful because of its ability to have a profile (vertical) image. Laptops and tablets both had good horizontal capability. Most patients don’t have a tripod for balancing the tablet, so they may need to be inventive with stacking books, a picture frame, etc., in order to balance the tablet. Both devices had to be moved to different levels in height to get the best angles. The floor, different chair heights, a stepping stool, dining room table and even a bed are suggestions to use to obtain a good camera angle, which is very important for proper visualization and instruction.
Lighting
- Try to have the patient perform the assessment exams and exercises against a blank wall with lighting behind the camera, such as a window with natural light. If natural light is not available, lamps and lighting behind the camera is often best.
Telemedicine Patient Assessment
Chief Complaint: 41 year-old female complains of persistent low back pain that is worse with activity such as walking long distances. It is worse in the morning upon waking, better with heat, and is an acute episode of a chronic low back issue.
Patient History: TCM Differential Diagnosis
- Ask the patient pertinent questions to help formulate the zang fu pattern that may be contributing to their pain. Assess the lateral view of the patient to observe if the patient’s posture is associated with a zang organ pathology. See later in this article under “Static Assessment – Lateral View” (SMAC students, refer to your Module I notes on “Posture and Zang Organ Pathology”).
- Examine the tongue. A good light source is important for this. If the patient has a white or pink colored paper/card accessible, placing the paper or card next to the patient’s tongue for color differentiation can be beneficial.
- How is the patient’s spirit? These challenging times and an injury can be emotionally and physically devastating. Consider treatment points to address any emotional components of the injury/patient. Prescribing appropriate exercises will enable the patient to take an active role in their healthcare, which in itself is good for the spirit. More than ever, now is a time for improving self-love. Balancing posture with exercises also enhances organ function, therefore exercise prescription will be very beneficial for your patients.
Description of Pain
Make sure to ask the patient to rate their pain on a scale of 1-10 during their first telemedicine visit.
- Where is the pain? Can the patient identify the location with their fingers? In this video, the patient describes her pain in different regions. The various assessment examinations also provoked the pain, which helps the practitioner to identify the possible structures that are involved in the pain pattern. With extension type movements (standing lumbar extension and stork standing test), the pain was on the midline (indicating possible facet joint irritation) and also on the right in the soft tissue regions (which indicates possible involvement of the lateral fibers of the iliocostalis, the lateral raphe and/or the quadratus lumborum). The practitioner could be anticipating an elevated ilium and possible anterior tilt with this information. This will be discussed in the Patient Assessment section below.
- If the pain is in a fixed region, consider injuries, such as yaoyan syndrome, lumbar facet joint pathology, sacroiliac joint and soft tissue strain, etc. The patient in the video indicates fixed regions of pain a few times after performing particular functional exams.
- Is the pain radiating? Does the patient describe a traveling sensation verbally or with their hand? In this case study, the patient traced from the upper lumbar/lower thoracic region toward the SI joint, deep gluteals, and also toward the greater trochanter. This body language would signal to the practitioner the possibility of thoracolumbar junction syndrome (TLJS) and possibly a radicular pain pattern. The primary assessment for TLJS is with motion palpation by the practitioner of the vertebrae at the T11-L1 region. Because this assessment is not an option under this current situation, a virtual examination is needed. The lumbopelvic rhythm test, positive in this case, can be helpful in this situation. To rule out the possibility of the patient’s pain being radicular (S1 dermatome in this case), have the patient perform a simple nerve tension test, the straight leg raise test (SLR). This examination is normally performed by the practitioner and is passive for the patient. For this telemedicine examination, the patient can perform the SLR on the affected side with hip flexion and a straight leg (be sure the exam is performed with the knee extended). Secondly, have the patient perform the SLR using a large towel placed around the ankle. The patient is asked to relax the leg as much as possible. The practitioner will need to verbally guide the patient step-by-step with this examination.
Static Postural Assessment
Posterior view:
- Observe for an elevated ilium. Be careful not to use the patient’s pant line as a measurement. In this case study, the patient seems to have an elevated ilium on the right (left pelvic tilt).
- Is there an L4-L5 vertebral tilt? This will help to reinforce an elevated ilium. The patient has a left L4-L5 tilt, which further indicates a right elevated ilium.
- Lateral tilt of the ribcage: Observe for a lateral tilt of the ribcage to the same side of the elevated ilium.
- Examining the lower extremity as part of the lumbopelvic assessment would also be useful, although this will be covered in a future blog and video.
Lateral View: L and R
- Posture and Zang Pathology Patterns: Exam for the five different body postures (A) and inquire with TCM questioning to help support the corresponding zang postural pattern. In the video, the patient has an anterior hip shift with the rest of the body in alignment. This particular posture is indicative of kidney qi deficiency and qi and blood deficiency. The practitioner should expect a pale, possibly swollen tongue body. The tongue coat is often thin. This particular posture (a frontal plane deviation) requires therapeutic exercise prescription, but it is also imperative to address the Kidney qi and the overall quality of qi and blood for these cases so that the postural changes hold and the low back pain subsides.
- Pelvic and Trunk Rotation: Examine the left and right innominate bones, hip joint and shoulders (acromion at LI 15). This patient has the right hip joint further forward than the left hip joint, which indicates a left pelvic rotation. At this point the practitioner may suspect a right trunk rotation as a compensation and this can be evaluated in the functional assessment. The torsion between the trunk and pelvis is very common in low back pain cases. The practitioner should be considering using points such as GB 41-SJ 5, SP 3 – ST 40. Refer to the Patient Treatment section later for more information.

Functional Assessment
- Observe the posterior view of the patient. Ask the patient to put their hands on their hips and move into trunk extension. Examine for quality of movement, tissue imbalances and pain. In this case, the patient indicates pain with this motion by placing a fist at the L2-L4 spinal region. This body language in extension types of movements often indicate facet joint injury. In the telemedicine video below, the practitioner can observe a bunching up of tissue in the lumbar region (L2-L4), which indicates possible swelling and facet joint irritation.
- Lumbopelvic Rhythm (lateral view): Examine for the innominate bone and spinal movements to be in sequence—does one segment move substantially more than the other segments? In the video, the practitioner can observe that the patient’s T12-L2 region moves posterior (extension) and does not move in coordination with the rest of the spine (moving into flexion). This unstable thoracolumbar junction coincides with the TLJS symptoms that the patient traced earlier in the video.
- Trunk Flexion (posterior view): Examine for imbalances in the pelvis. Observe for lumbar rotation as this can indicate an imbalance in the psoas muscles and Kidney jingjin.
- Seated Rotation: Have the patient place their arms to the side and rotate the trunk to the left and to the right. Is there restriction of movement? Does it match what the practitioner observed with pelvic rotation in the standing lateral view? In the video, the patient has left pelvic rotation and with this seated position has right trunk rotation. Typically, the patient will have more difficulty rotating in the direction of the pelvic rotation due to the counter-rotation in the trunk.
- Stork Standing Test: Have the patient use a nearby wall or chair to help balance themselves during this exam. We are using this test to challenge the lumbar facet joints, which we suspect may be contributing to some of the patient’s pain. In the video, the patient felt pain in the soft tissues lateral to the L2-L4 vertebrae and indicated with her fist the lateral iliocostalis fibers, the lateral raphae and quadratus lumborum region. The practitioner could consider the affected sinew channels and points to relieve patient’s pain. These points could include the accumulating (xi-cleft) and connecting (luo) points on the iliocostalis – UB, lateral raphe – ST, and quadratus lumborum – LIV channels.
- Thoracolumbar Fascia Rotation Test: This is a good choice in examinations when pelvic/trunk rotation is suspected in a patient with low back pain. This test examines the tissue relationship between the latissimus dorsi, the thoracolumbar fascia (TLF) and the contralateral gluteus maximus. In this case study, the patient had bilateral limited trunk rotation indicating locked-short latissimus dorsi, worse when rotating to the left. This thoracic rotation increased when the left gluteus maximus was activated. The practitioner should consider treatment of the right latissimus dorsi, left gluteus maximus, the TLF and possible thoracic vertebral fixations contributing to zang fu pathology.
- Gillet’s Test: Describe to the patient how to perform hip flexion (to 90˚-100˚). Observe the patient from the posterior view as they perform this motion and watch the hip and innominate motion. In this video, the patient seems to have a left positive Gillet’s sign. The practitioner will use GB 41-SJ 5 on the left prior to performing the exercises later.
- FABER—Seated and supine: Record the findings of where the pain is located. In the video, the patient indicates pain in the gluteus medius/minimus region and also in the psoas lower attachment, the ligamentous hip joint capsule may also be involved.
- Sacroiliac Rocking Test: We used this test to challenge the sacroiliac joint. The test was negative, but did indicate pain in the psoas region and possibly in the hip joint capsule.
- Overhead Squat (OHS) posterior view: Is there an asymmetrical hip shift? This hip shift is often to the same side as the elevated ilium. Remotely, we can help to correct this imbalance through acupressure on specific points in addition to specific exercises to tissues associated with the LIV and GB myofascial jingjin channels of the pelvis. Refer to the exercises later in this blog. In this video, the patient after some coaching on how to distribute her body-weight during the exercise showed a right asymmetrical hip shift toward the end range of the movement.
- OHS lateral view: Look for arms falling forward, excessive forward lean, lumbar hyperextension or flexion. This particular movement was not performed in this video, although it could be used as a follow-up assessment on the second visit. It is suspected that the patient will have arms falling forward and/or excessive hyperextension.
Diagnosis
- Kidney qi and qi and blood deficiency
- Right elevated ilium and associated myofascial channel imbalances
- Left pelvic rotation and right trunk rotation
- Bilateral anterior pelvic tilt (more on the right)
- Possible thoracolumbar junction syndrome
- L2-L4 region facet joint injury
Treatment Plan (Initial Visit)
- Strengthen Kidney qi and systemic qi and blood
- Balance the postural deviations
- Decrease pain in the UB, ST and LIV jingjin of the low back
Treatment Protocol
Diagnosing the patient’s internal pathology with a TCM differential diagnosis inquiring is imperative. Underlying conditions can be addressed through acupressure prescriptions, dietary recommendations and Chinese herbal medicine. Qi gong exercises are a great compliment to strengthening the body and to balance qi and blood. See the resources at the end of this blog for online qi gong and tai chi classes.
Acupressure Points
The following list of acupuncture and motor points are a combination of points to address the patient’s constitution, their postural misalignments and their pain.
The points are to be stimulated by the patient with digital pressure. It is best for the patient to stimulate these points 2x/day and especially important to stimulate them prior to performing the prescribed exercise routine. Manual stimulation to the points can be applied with many different tools, the fingertip or massage tools are suggestions.
Ask the patient to apply a downward pressure with small circular motions (circumference of 0.25 inch) examining for painful areas or restricted tissues. Massage for 5-10 seconds. Next, apply the finger or massage tool into the point, at a 45˚-75˚ angle and push the tissue away firmly in four or more directions, holding each direction for 5-10 seconds.
The following are suggestions of points for acupressure:
- GB 41-SJ 5 – on the left (positive Gillet’s test)
- K3-K4 – bilateral, as this helps to significantly decrease pain from lumbar facet joint injury
- SP 3-ST 40 – this source/luo point combination helps to balance the internal and external obliques
- UB 58, LIV 5, ST 40 – luo points for the UB, LIV and ST channels
- GB 39.5-LIV 4 — for the right innominate bone that has the greatest anterior pelvic tilt
- LIV 3, P6, SP 6, ST 36 and LI 10 – this classic point combination helps to move liver qi, calm the spirit and tonify qi and blood
- UB 22-24 region with yoga tune-up balls (This will help to activate the renal fascia that surrounds the kidney and to loosen the low back soft tissue that is constricted from the bilateral anterior tilt.)
- Piriformis motor point bilateral with yoga tune-up balls. (This will help to activate a “binding region” of the UB jingjin and also help with pelvic balancing and decreasing local pain.)
Exercises (Initial Telemedicine Visit)
The following information is from the Postural Assessment and Corrective Exercise (PACE) portion of the SMAC Program. These exercises are also covered in the Sports Medicine Acupuncture textbook. This exercise prescription is based on the patient diagnosis in the accompanying telemedicine video to this blog. This exercise prescription is not intended for use in all cases of low back pain.
For this initial telemedicine visit, we decided to prioritize balancing the bilateral anterior pelvic tilt (frontal plane deviation), elevated ilium (transverse plane deviation), pelvic and trunk rotation (frontal plane deviation). Helping to balance these structural deviations by activating the UB/K, LIV/GB and SP/ST myofascial sinew channels can help to quickly decrease the patient’s pain. As discussed previously, having the patient apply acupressure massage to the suggested points just prior to exercise helps with the proprioceptive signaling of these myofascial channels, which can increase the benefit of these exercises.
Exercise Routine (initial telemedicine visit)
- Static Back Position (FR at knees)
- Double-Knee to Chest
- Hip Adductors (FR or YTB): Same side as the elevated ilium
- Hip Adductor Stretch: Same side as the elevated ilium
- Clam Shells: Same side as the elevated ilium
- Hip Abductors (FR or YTB): Opposite side as the elevated ilium
- Gluteal Stretch: Opposite side as the elevated ilium
- Inner Leg Lifts: Opposite side as the elevated ilium
- Latissimus dorsi (FR)
- Figure 4 Spinal Rotation
- Psoas Stretch
- Dead Bug
- Wall-Sit (FR)
Key:
Foam Roll (FR)
Yoga Tune-up Balls (YTB)
Exercise Routine Rationale
This section will help to explain the reasoning behind this exercise routine.
NOTE: As discussed in the SMAC program, when the practitioner uses acupuncture prior to the exercise routine, the amount of prescribed exercises will be less. In this case, because acupuncture stimulation is not being used, the number of exercises prescribed is increased in order to reinforce the treatment plan.
- Static Back Position (FR at knees) – Passively relaxes the UB and K jingjin. This is a good beginning exercise to help the body rest and align in a neutral position. By gently contracting the adductors (LIV jingjin), the line of pull by this muscle group onto the pelvis further decreases the anterior tilt.
- Double-Knee to Chest – Actively opens the UB and K myofascial jingjin of the low back and spine. Passively relaxes the imbalanced SP and ST jingjin of the abdomen.
- Hip Adductors (FR and/or YTB) on same side of elevated ilium — Reduces excess in the LIV channel (adductors).
- Hip Adductor Stretch on same side of elevated ilium — Elongates and further reduces the LIV channel (adductors) and signals the GB jingjin (hip abductors).
- Clam Shells on same side of elevated ilium — Activates the GB jingjin and relaxes the LIV jingjin.
- Hip Abductors (FR and/or YTB) on opposite side of elevated ilium — Reduces excess in the GB channel (hip abductors).
- Gluteal Stretch on opposite side of elevated ilium — Elongates and further reduces the GB channel (hip abductors) and signals the LIV jingjin (adductors).
- Inner Leg Lifts on opposite side of elevated ilium — Activates the LIV jingjin and relaxes the GB jingjin.
- Latissimus dorsi (FR) — This exercise softens the excess and locked-short fibers of the UB jingjin with the upper half of the latissimus dorsi.
- Figure 4 Spinal Rotation — This is an excellent exercise for decreasing an elevated ilium. The patient begins the exercise with the active leg on the same side of the elevated ilium. This exercise coordinates the hip abductors (GB jingjin) that are locked-long and in a relative deficient condition with the hip adductors (LIV jingjin) that are locked-short and in a relative excess condition. The activation of the hip abductors will reciprocally inhibit the hip adductors, which is beneficial in decreasing the elevated ilium.
- Psoas Stretch — Elongates the locked-short psoas fibers and Kidney jingjin. By stretching these fibers the UB jingjin of the low back is signaled.
- Dead Bug — This core stabilization exercise is placed toward the end of the routine and is designed to activate and coordinate the imbalanced jingjin and to reinforce the entire routine. SP, ST and K jingjin are strongly emphasized in this exercise.
- Wall-Sit (with FR) — This exercise, like the first exercise in this routine, is activating the adductors to help reduce the bilateral anterior tilt. This exercise is good to place last in the routine as it helps to align the body and lock in the previous movement patterns.
Individual Exercises
Click on the + to see an image and instructions for each of the individual exercises used in this telemedicine case study.

Static Back Position
- Patient Position: The supine patient is positioned with the hips and knees flexed to 90° resting on a chair. Arms are abducted to 90° with the palms down. This position neutralizes the pelvis and spine.
- Procedure: For a bilateral anterior tilt, a foam roll can be placed between the knees (not shown on image). Gently contract the adductors (LIV jingjin) to help decrease the increased lordotic curve of the patient’s back.
- Sets: 3
- Repetitions: 30 seconds
- Breathing: Slow deep breaths. Three deep breaths between sets. Be sure patient is instructed to breathe diaphragmatically into the dan tian.

Double Knee to Chest
- Patient Position: Supine patient holding knees to chest with both hands.
- Procedure: Supine patient holding knees to chest with both hands increasing stretch as muscles relax.
- Sets: 3
- Repetitions: 30 seconds
- Breathing: Slow deep breaths. Three deep breaths between sets. Be sure patient is instructed to breathe diaphragmatically into the dan tian.

Hip Adductor
(foam roll or yoga tune-up ball)
This exercise is performed on the same side as the patient’s elevated ilium.
- Patient Position: Patient is instructed to lie prone and hold themselves up on their elbows with the forearms placed onto the floor. A foam roll is placed into adductor region of one leg, the knee is bent and the foot is kept off the foam roll.
- Procedure: Patient is instructed to slowly roll the inner thigh along the Liver and Spleen channels starting from the LIV 10 down toward the medial knee. The patient is instructed to locate and stop at ashi points.
- Sets: 1
- Repetitions: Hold 30 seconds per ashi point
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Resting the foot on the floor or not having the foam roller perpendicular to the thigh.
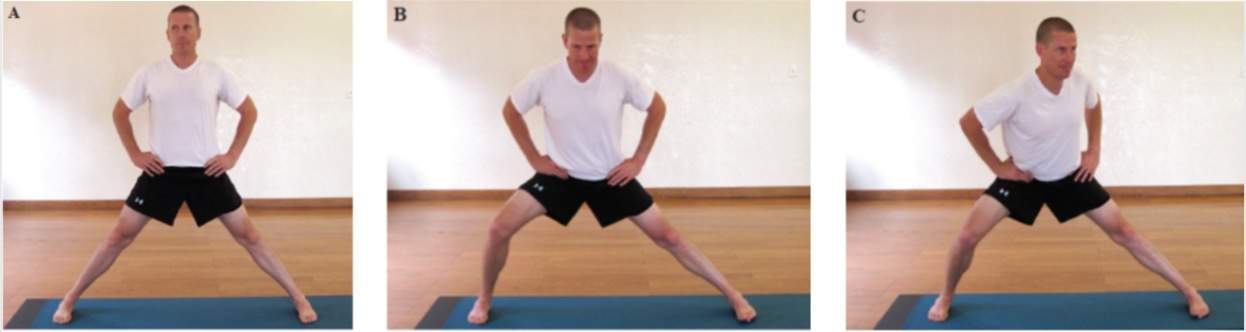
Hip Adductor Stretch
This exercise is performed on the same side as the patient’s elevated ilium.
- Patient Position: Patient stands with legs wider than shoulder-width apart. The feet are pointed straight ahead and hands on the hips (A).
- Procedure:Patient is instructed to shift their body-weight onto the opposite side, keeping the other leg straight until a stretch is felt in the inner thigh (B). The patient then rotates the hips in the direction of the straight leg feeling for a stretch in the posterior adductor fibers (C). Both feet must always remain pointing forward.
- Sets: 1
- Repetitions: Hold stretch for 30-60 seconds
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Letting the bent knee go farther forward than the toes.

Clam Shells
This exercise is performed on the same side as the patient’s elevated ilium.
- Patient Position: Patient is in a side-lying position with the bottom arm fully abducted forming a straight line with the trunk and hips. Hips are flexed to 45° with one leg on top of the other, aligning the knees and ankles together.
- Procedure:The patient is instructed to raise the top knee into hip abduction to a level of 30-45°. The knee is then lowered back down slowly.
- Sets: 2
- Repetitions: 10
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Not keeping the pelvis vertical.

Hip Abductors
(foam roll or yoga tune-up ball)
This exercise is performed on the opposite side of the patient’s elevated ilium.
- Patient Position: The patient is sitting on the foam roll with one foot crossed over the other knee. The stabilizing leg is bent to 90° and the foot is on the floor.
- Procedure: Patient is instructed to slowly roll the lateral hip applying pressure on ashi points in the following directions: 1) Between the greater trochanter and the iliac crest, 2) Between the greater trochanter and the sacroiliac joint.
- Sets: 1
- Repetitions: Hold 30 seconds per ashi point
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Rolling onto the greater trochanter, rolling on the side of the planted leg (rolling on the wrong hip).

Gluteal Stretch
This exercise is performed on the opposite side of the patient’s elevated ilium.
- Patient Position: The patient starts from a supine position and brings one lower extremity across the midline into hip adduction while rotating the head to the opposite side. The knee of the adducted hip is flexed as it is placed into approximately 45˚-90˚ of hip flexion in order to stretch the gluteus medius/minimus muscles.
- Procedure: The patient can stabilize and increase the stretch by pressing down on the knee. Hold this position for 30-60 seconds before progressing to the next step (A). The patient then flexes the hip further by bringing the knee toward the armpit. The patient can use their hand to stabilize and increase the stretch to ensure that it is felt in the lower fibers of the gluteus maximus (B).
- Sets: 1
- Repetitions: Hold 30-60 seconds per position
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.

Inner Leg Lifts
This exercise is performed on the opposite side of the patient’s elevated ilium.
- Patient Position: Patient is in a side-lying position with the bottom arm fully abducted forming a straight line with the trunk and hips. The bottom leg is placed into 10 -15° of hip flexion, knee extension and foot dorsiflexion. The hip of the top leg is flexed and externally rotated so the foot is on the floor in front of the pelvis. Patient is instructed to hold the ankle with the top arm for stability.
- Procedure: The bottom leg is adducted as high as possible while maintaining 10 -15° of hip flexion and then lowered.
- Sets: 2
- Repetitions: 10
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically and expand the dan tian.
- Compensation: Trunk flexion. Not keeping the pelvis vertical and the foot parallel to the floor due to hip rotation.

Latissimus dorsi
(foam roll or yoga tune-up ball)
The patient uses the FR or YTB on the opposite side of the limited trunk rotation as found in the thoracolumbar fascia rotation test. For example, if trunk rotation is limited when moving to the right then the left latissimus dorsi would be treated.
- Patient Position: Patient on side in lateral recumbent position with arm nearest floor held overhead in shoulder external rotation and thumb pointed toward ceiling. A 6” foam roll is placed under superior aspect of latissimus dorsi located slightly posterior to the Spleen channel points SP 18 – SP 20.
- Procedure: Patient on the foam roll moves body up and down the latissimus dorsi feeling for tender areas (ashi points). Once the ashi points are located, the patient is instructed to stay in this position for 30 seconds.
- Sets: 2
- Repetitions: 30 seconds per ashi point
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Spinal rotation off of latissimus dorsi.
Figure 4 Spinal Rotation
An excellent exercise for decreasing an elevated ilium.
 Patient Position: While lying on the floor in a supine position, the patient flexes both knees to 90˚ with the feet placed on the floor in a neutral position in alignment with the hip joints. One leg is placed into a Figure 4 position so that the lateral malleolus is placed onto the distal thigh of the opposite leg near the extra point heding. The shoulders are abducted to 90˚ with the palms down (A).
Patient Position: While lying on the floor in a supine position, the patient flexes both knees to 90˚ with the feet placed on the floor in a neutral position in alignment with the hip joints. One leg is placed into a Figure 4 position so that the lateral malleolus is placed onto the distal thigh of the opposite leg near the extra point heding. The shoulders are abducted to 90˚ with the palms down (A).- Procedure: While maintaining the Figure 4 position, the patient rotates the lumbar spine so that the foot of the Figure 4 leg reaches the floor. The bottom of the foot needs to be placed so that the K 1 region and heel are on the floor. The lateral aspect of the opposite thigh and leg should be resting on the floor. If it is comfortable for the patient’s neck, they can turn their head to the side opposite of the lumbar spine rotation. The patient is instructed to use their hip muscles to push the knee of the Figure 4 leg outward. The lateral malleolus of the Figure 4 leg must not move away from its placement on the distal femur. The patient is actively using the gluteal muscles to externally rotate, abduct and extend the hip joint, thereby passively stretching the soft tissue attachments on the greater trochanter (B).
- Sets: 1
- Repetitions: Hold for 30 – 60 seconds per side. Begin on the side of the elevated ilium, which is the same side with the foot that is on the floor. Repeat to the opposite side and then repeat a third time to the initial position.
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.

Psoas Stretch
- Patient Position: Kneeling on back leg, the patient is instructed to place the opposite leg forward with 90° of knee flexion and the toes pointing forward.
- Procedure: Patient is instructed to squeeze the gluteals to shift hips forward feeling for a stretch in the anterior hip. The knee of the forward leg should not move past the toes. Keeping the trunk upright. The arm on the side being stretched is extended overhead increasing lumbar lordosis and thereby further stretching the psoas.
- Sets: 2
- Repetitions: 30 seconds per ashi point
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Spinal rotation off of latissimus dorsi.

Dead Bug
- Patient Position: The supine patient has both arms extended toward the ceiling, directly over the shoulders, hips and knees are bent to 90°, the calves are parallel to floor with the ankles dorsiflexed. The back is flattened by engaging the abdominal muscles to create a posterior pelvic tilt. Keeping the shoulders down and ankles dorsiflexed, the abdominal core engaged. Extend your right arm and left leg away from you.
- Procedure: The patient is instructed to keep the low back flat on the floor while extending the opposite arm and leg, repeat to the opposite side. This exercise can be enhanced by activating the pelvic floor. The patient is asked to begin the exercise by bringing their REN 1 region superior and then performing the exercise.
- Sets: 3
- Repetitions: 20
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Lower or upper back arching off of the floor.
Wall-Sit (foam roll)
This exercise is good to place last in the routine as it helps to align the body and lock in the previous movement patterns.
 Patient Position: Patient’s back is flat against the wall; the hips and knees are flexed to 90°. Feet are in neutral position with lower extremities hip-width apart. Arms are held comfortably to the side. Foam roll is placed between the knees.
Patient Position: Patient’s back is flat against the wall; the hips and knees are flexed to 90°. Feet are in neutral position with lower extremities hip-width apart. Arms are held comfortably to the side. Foam roll is placed between the knees.- Procedure: Have the patient squeeze the knees against the foam roll while maintaining correct alignment of the legs.
- Sets: 1
- Repetitions: 30 seconds – 2 minutes
- Breathing: Slow deep breaths. Be sure patient is instructed to breathe diaphragmatically into the dan tian.
- Compensation: Holding the breath.
Prognosis
During the second telemedicine visit, re-examine all postural, orthopedic and functional exams and compare to the initial telemedicine visit for improvement in range of motion, nature and quality of pain. All exams should be 20-50% better in pain level if the diagnosis was correct. It is a positive sign if the pain starts to centralize, i.e. the patient experiences more fixed region pain that becomes more central and not peripheral. It is also positive if the patient expresses that there is less migrating or traveling pain. These are all signs of improvement. Inquire if the patient has received and is taking the Chinese herbal formula that was prescribed. How are the dietary changes coming along?
Depending on the postural changes that were achieved, the self-acupressure, self-massage and therapeutic exercises can be modified to match the internal and structural changes.
In Gratitude
Thank you to Brian Lau, Lesley Spencer, Lili Gould, Adam Schreiber and Patricia Botet for their contributions in getting this telemedicine project out so quickly and efficiently. A huge thank you for this gratis effort and vision to support licensed acupuncturists.
Resources
- Sports Medicine Acupuncture Certification Program
- Sports Medicine Acupuncture: An Integrated Approach using Sports Medicine with Traditional Chinese Medicine
- Ideal Balance: Brian Lau online qi gong and tai chi classes
- Yoga Tune-up Balls
- Foam rolls – There are many different distributors that can be found online
About the author(s):

Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.

Brian Lau, AP, C.SMA is has been on the faculty of the Sports Medicine Acupuncture Certification since 2014, and also teaches foundation courses with AcuSport Education. Brian lives and practices in Tampa, FL where he owns and operates Ideal Balance: Center for Sports Medicine Acupuncture (www.ideal-balance.net). He blogs on anatomy and TCM at www.sinewchannels.com.
About the author(s):
Matt Callison is the president of the Sports Medicine Acupuncture Certification program. He has been combining sports medicine and traditional Chinese medicine (TCM) for over 26 years. He is the author of the Motor Point and Acupuncture Meridians Chart, the Motor Point Index, The Sports Medicine Acupuncture textbook and many articles on the combination of sports medicine and TCM.
Brian Lau, AP, C.SMA is has been on the faculty of the Sports Medicine Acupuncture Certification since 2014, and also teaches foundation courses with AcuSport Education. Brian lives and practices in Tampa, FL where he owns and operates Ideal Balance: Center for Sports Medicine Acupuncture (www.ideal-balance.net). He blogs on anatomy and TCM at www.sinewchannels.com.